 for Acute Myocarditis")
Overview
Cardiol Therapeutics (NASDAQ:CRDL,TSX:CRDL) is a clinical-stage life sciences company focused on the research and clinical development of anti-inflammatory and anti-fibrotic therapies for the treatment of heart disease. The company’s lead small molecule drug candidate, CardiolRx (cannabidiol) oral solution, is pharmaceutically manufactured and in clinical development for use in the treatment of heart disease. It is recognized that cannabidiol inhibits activation of the inflammasome pathway, an intracellular process known to play an important role in the development and progression of inflammation and fibrosis associated with myocarditis, pericarditis and heart failure.
Cardiol has received Investigational New Drug Application authorization from the United States Food and Drug Administration to conduct clinical studies to evaluate the efficacy and safety of CardiolRx in two diseases affecting the heart: (i) a Phase II multi-center open-label pilot study in recurrent pericarditis (the MAvERIC-Pilot study; NCT05494788), an inflammatory disease of the pericardium which is associated with symptoms including debilitating chest pain, shortness of breath, and fatigue, and results in physical limitations, reduced quality of life, emergency department visits, and hospitalizations; and (ii) a Phase II multi-national, randomized, double-blind, placebo-controlled trial (the ARCHER trial; NCT05180240) in acute myocarditis, an important cause of acute and fulminant heart failure in young adults and a leading cause of sudden cardiac death in people less than 35 years of age.
Cardiol is also developing a novel subcutaneously administered drug formulation of cannabidiol intended for use in heart failure – a leading cause of death and hospitalization in the developed world, with associated healthcare costs in the United States exceeding $30 billion annually.
Company Highlights
- Lead Asset in Clinical Development: CardiolRx, oral drug candidate, in Phase II trials for recurrent pericarditis and acute myocarditis.
- Scientific Rationale: Compelling evidence demonstrating the anti-inflammatory and antifibrotic properties of CardiolRx in myopericardial diseases.
- Innovative Research: Advancing the development of CRD-38, a novel proprietary subcutaneously administered pharmaceutical intended for use in heart failure.
- CRD-38 Positive Study Results: Positive study results demonstrating CRD-38 subcutaneous formulation slowed increases in body weight and heart weight, and prevented increases in key cardiac inflammatory and remodeling markers in a model of heart failure with preserved ejection fraction.
- Broad Exclusivity Protection: Comprehensive intellectual property portfolio. Eligible to pursue FDA orphan drug and EMA orphan medicine designations for CardiolRx.
- Leadership: Experienced management team, board of directors, and scientific advisory board, with extensive expertise in developing therapeutics for inflammatory heart disease.
- Strong Financial Position: Debt-free and well-capitalized to achieve corporate milestones into 2026.
Key Projects
Orphan Drug Program for Recurrent Pericarditis
In November 2023, Cardiol announced that it has exceeded 50 percent of the patient enrollment target for the company-sponsored Phase II open-label MAvERIC-Pilot study investigating the tolerance, safety and efficacy of CardiolRx in patients with recurrent pericarditis. The study will also assess the improvement in objective measures of disease, and during an extension period, assess the feasibility of weaning concomitant background therapy including corticosteroids, while taking CardiolRx.
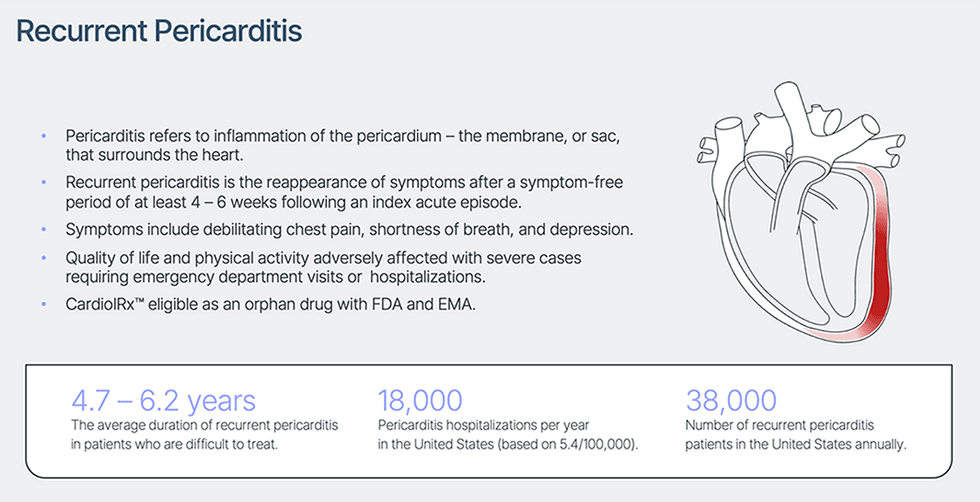
Pericarditis refers to inflammation of the membrane or sac that surrounds the heart (the pericardium) that is most frequently triggered by a viral infection. Recurrent pericarditis is the most common complication following an initial acute episode of pericarditis, and patients may have multiple recurrences. Symptoms include debilitating chest pain, shortness of breath, and fatigue, resulting in physical limitations, reduced quality of life, emergency department visits, and hospitalizations. Infrequent but life-threatening complications associated with pericarditis include a large accumulation of pericardial fluid, scarring, and constriction of the heart which may limit heart function. The disease is diagnosed in 0.2 percent of all cardiovascular in-hospital admissions and is responsible for 5 percent of emergency room admissions for chest pain in North America and Western Europe. Recurrent pericarditis is the re-appearance of symptoms after a symptom-free period of at least 4 – 6 weeks following an initial acute episode of pericarditis. These recurrences appear in 15 percent to 30 percent of acute cases and usually within 18 months. Furthermore, up to 50 percent of patients with a recurrent episode of pericarditis experience more recurrences. Standard first-line medical therapy consists of non-steroidal anti-inflammatory drugs or aspirin with or without colchicine. Corticosteroids such as prednisone are second-line therapy in patients with continued recurrence and inadequate response to conventional therapy.
The only FDA-approved therapy for recurrent pericarditis, launched in 2021, is generally used as a third-line intervention in patients with a third or fourth recurrence. The number of cases of patients seeking and receiving treatment for recurrent pericarditis annually in the US is estimated at 38,000. Hospitalization due to recurrent pericarditis is often associated with a 5 – 8 day length of stay and cost per stay is estimated to range between $20,000 and $30,000 in the United States.
The Phase II MAvERIC-Pilot study is expected to enroll 25 patients at clinical centers in the United States that specialize in pericarditis care. The protocol has been designed in collaboration with thought leaders in pericardial disease. The study chairman is Dr. Allan L. Klein, director of the Center of Pericardial Diseases and professor of medicine, at the Heart and Vascular Institute at the Cleveland Clinic. The primary efficacy endpoint is the change, from baseline to eight weeks, in patient-reported pericarditis pain using an 11-point numeric rating scale (NRS). The NRS is a validated clinical tool employed across multiple conditions with acute and chronic pain, including previous studies of recurrent pericarditis. Additional endpoints during the extension period include the NRS score after 26 weeks of treatment, and changes in inflammatory marker C-reactive protein (CRP), a commonly used clinical marker of inflammation.
“Recurrent pericarditis is a debilitating inflammatory heart disease associated with symptoms that adversely affect quality of life and physical activity. Results of the MAvERIC-Pilot study will assist in further understanding the therapeutic profile of our lead investigational drug in this condition and inform the design of a pivotal Phase III clinical trial to underpin the potential regulatory approval of CardiolRx, which is also being evaluated in the global ARCHER Phase II trial in patients presenting with acute myocarditis,” said David Elsley, Cardiol Therapeutics’ president and chief executive officer.
In the US, an orphan drug designation is granted for pharmaceuticals being developed to treat medical conditions affecting fewer than 200,000 people. These conditions are referred to as orphan diseases. The assignment of orphan status to a disease and to drugs developed to treat it is a matter of public policy in many countries and has yielded medical breakthroughs that might not otherwise have been achieved. In the US and the European Union, orphan drugs are eligible for accelerated marketing approvals and companies developing orphan drugs typically receive other incentives, including a prolonged period of market exclusivity that can extend over seven years, during which the drug developer has sole rights to market the drug.
Recurrent pericarditis is an orphan disease in the United States, thereby making CardiolRx eligible for orphan drug status under the FDA’s Orphan Drug Designation program.
Independent advisors and key investigators comprising six highly distinguished thought leaders in cardiology from the Cleveland Clinic, the Mayo Clinic, the Monash Victoria Heart Institute, the University of Virginia, and Northwestern University have been established to design, oversee, and guide Cardiol’s Phase II MAvERIC-Pilot study in patients with recurrent pericarditis.
Orphan Drug Program for Acute Myocarditis
In January 2024, Cardiol exceeded 50 percent patient enrollment in ARCHER, the company’s Phase II multi-center, international, double-blind, randomized, placebo-controlled trial designed to study the safety and tolerability of CardiolRx, as well as its impact on myocardial recovery, in patients presenting with acute myocarditis.
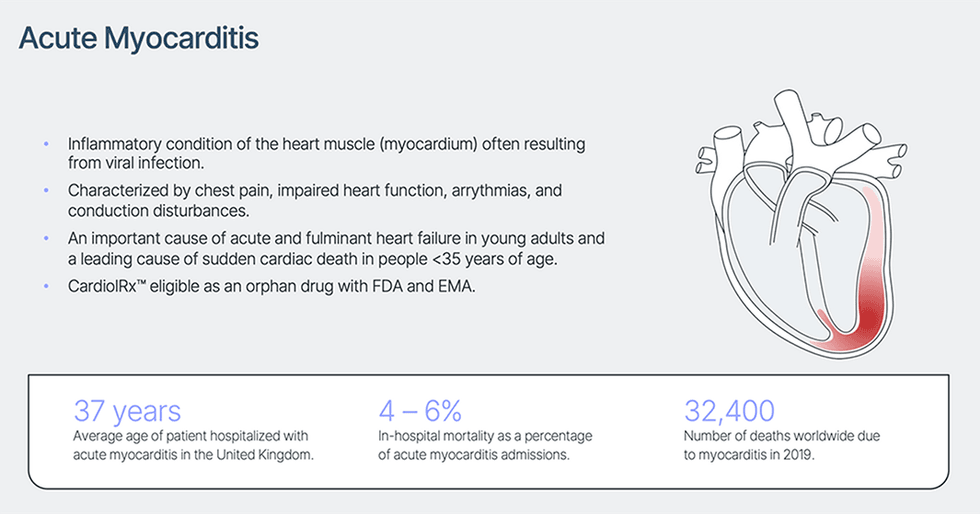
Myocarditis is an acute inflammatory condition of the heart muscle (myocardium) characterized by chest pain, impaired cardiac function, atrial and ventricular arrhythmias, and conduction disturbances. Although the symptoms are often mild, myocarditis remains an important cause of acute and fulminant heart failure and is a leading cause of sudden cardiac death in people under 35 years of age. Although viral infection is the most common cause of myocarditis, the condition can also result from bacterial infection, commonly used drugs and mRNA vaccines, as well as therapies used to treat several common cancers, including chemo-therapeutic agents and immune checkpoint inhibitors.
In a proportion of patients, the inflammation in the heart persists and causes decreased heart function with symptoms and signs of heart failure, and as such treatment is based on standard-of-care recommendations for heart failure. This includes diuretics, ACE inhibitors, angiotensin receptors blockers, beta-blockers, and aldosterone inhibitors. For those with a fulminant presentation, intensive care is often required, with the use of inotropic medications (to increase the force of the heart muscle contraction). Severe cases frequently require ventricular assist devices or extracorporeal oxygenation and may necessitate heart transplantation.
There are no FDA-approved therapies for acute myocarditis. Patients hospitalized with the condition experience an average 7-day length of stay and a 4 – 6 percent risk of in-hospital mortality, with average hospital charge per stay estimated at $110,000 in the United States.
“The US orphan drug program was successfully utilized to accelerate the first FDA approval of CBD for the treatment of rare forms of pediatric epilepsy, and significant shareholder value was created in the process,” Elsley said. “Given the mortality and significant morbidity risk associated with acute myocarditis, we believe there is a similar opportunity in pursuing an expedited development program of our CardiolRx pharmaceutical CBD formulation for this serious orphan disease which has no accepted standard of care.”
The primary efficacy endpoints of the Phase II ARCHER trial consist of extracellular volume (ECV) and global longitudinal strain (GLS). The secondary efficacy endpoint is left ventricular ejection fraction. Since people with acute myocarditis have impaired heart function, current treatment is based on standard-of-care recommendations for heart failure. This includes diuretics, ACE inhibitors, angiotensin receptors blockers, beta-blockers, and aldosterone inhibitors. For those with a severe and sudden onset presentation, intensive care is often required, with the use of inotropic medications (to increase the force of the heart muscle contraction) and occasionally, heart-lung bypass or ventricular assist devices. There is otherwise no specific treatment for acute myocarditis although some patients have responded to immuno-suppressive therapy (azathioprine) in combination with steroids, but the data are not conclusive enough for this to be the recommended therapy.
An independent clinical steering committee, comprising 10 highly distinguished thought leaders in cardiology from the Cleveland Clinic, the Mayo Clinic, the Houston Methodist DeBakey Heart and Vascular Center, the University of Ottawa Heart Institute, McGill University Health Centre, the University of Pittsburgh Medical Center, University Medicine Berlin, Tel Aviv “Sourasky” Medical Center, São Paulo University Medical School, and Pitié Salpêtrière Hospital (Sorbonne University), has been established to design, oversee, and guide Cardiol’s Phase II multi-national ARCHER trial in acute myocarditis.
Cardiol Therapeutics’ Heart Failure Program
Heart failure affects more than 64 million people globally and associated healthcare costs exceed $30 billion annually in the US alone. Heart failure is a chronic, progressive syndrome in which the heart muscle is unable to pump enough blood to meet the body’s needs for blood and oxygen. People with heart failure suffer from shortness of breath, rapid heart rate, edema, reduced exercise capacity, often struggle with simple daily activities and are frequently hospitalized. For many, these symptoms significantly reduce their quality of life. Known causes of heart failure include ischemic heart disease and myocardial infarction (heart attack), hypertension, valvular heart disease, inflammatory diseases of the heart such as myocarditis and cardiomyopathies, anti-cancer therapies, and inherited metabolic diseases.
Heart failure remains a leading cause of morbidity and mortality worldwide and persists as a growing health and economic burden. In the United States alone, 6 million people over the age of 20 are living with heart failure, and this number is projected to increase to more than 8 million by 2030. The total annual cost attributed to heart failure is projected to increase to $69.8 billion by 2030.
Total deaths attributed to heart failure annually in the United States have been reported in the range of 86,000 to more than 300,000, and hospitalizations range from 800,000 to 1.3 million. The five-year mortality rate for those with heart failure has been reported at 52.6 percent overall.
Cardiol is developing CRD-38, a novel proprietary drug formulation designed to deliver cannabidiol by subcutaneous administration. They are undertaking IND-enabling activities to support clinical evaluation of CRD-38 as a therapeutic strategy in heart failure care – a leading cause of death and hospitalization in the developed world, with associated healthcare costs in the United States exceeding $30 billion annually.
In 2023, Cardiol announced positive study results from one of its international collaborating research centers indicating how the CRD-38 subcutaneous formulation slowed increases in body weight and heart weight and prevented increases in key cardiac inflammatory and remodeling markers in a model of heart failure with preserved ejection fraction.

Published third-party research has shown that cannabidiol reduces inflammatory activation of the endothelial lining of blood vessels and aids endothelial vasorelaxation, resulting in improved blood flow. Cannabidiol has also been shown to attenuate several measures of inflammation in models of diabetes, a common comorbidity in heart failure patients, and to reduce myocardial fibrosis in a model of inflammatory heart disease.
Cannabidiol is lipid soluble, virtually insoluble in water, highly sensitive to deactivation in the liver via first-pass metabolism when taken orally and is rapidly cleared from the body. This results in a low overall bioavailability when taken orally. Cardiol’s subcutaneously administered drug formulation is designed to minimize first-pass metabolism, optimize and maintain blood levels of the drug, and target inflammation and increased fibrosis in the heart. Cardiol believes that overcoming the low bioavailability issues associated with cannabidiol will significantly broaden the therapeutic potential of this molecule.
Cardiol Therapeutics’ Key Global Research and Clinical Collaborators
Cardiol is working together with world-class researchers and clinicians at international centers of excellence to leverage their expertise in drug development, experimental execution, inflammation and fibrosis, the treatment of cardiovascular diseases, and clinical trial protocol design. The collaborations provide optimal advice and knowledge platform in pursuit of Cardiol’s purpose: to heal the heart with innovative science.

Management Team
David Elsley – President, Chief Executive Officer, and Director
David Elsley is the founder and CEO of Vasogen and has an MBA degree. Elsley has over 25 years of experience developing, financing, and managing all aspects of corporate development in biotechnology and high-growth organizations. Elsley founded Vasogen, a biotechnology company focused on the research and commercial development of novel therapeutics for the treatment of heart failure and other inflammatory conditions. Elsley assembled a team of management, directors and scientific advisors comprising industry professionals and thought leaders from North America and Europe.
Dr. Andrew Hamer – Chief Medical Officer and Head of Research and Development
Dr. Andrew Hamer has an MBChB degree. He is the former executive director at Amgen, responsible for leading global development of Repatha®. Hamer is the former chief cardiologist at Nelson Hospital, New Zealand. He has over 19 years of experience practicing cardiology and internal medicine.
Chris Waddick – Chief Financial Officer and Director
Chris Waddick has an MBA degree, is a chartered professional accountant, and is a certified management accountant. He has over 30 years of experience in financial and executive roles in the biotechnology and energy industries. Waddick is the former chief financial officer and chief operating officer of Vasogen Inc.
Bernard Lim – Chief Operating Officer
Bernard Lim has over 30 years of experience in the life sciences industry, spanning biotechnology, diagnostics, medical devices, and high-technology companies. He is the founder and CEO of a highly successful drug delivery company that he led from research and development through to commercialization, and facilitated its eventual acquisition by Eli Lily. Lim is a chartered engineer per UK standards and is a member of the Institution of Engineering and Technology.
Andrea B. Parker – Senior Director of Clinical Operations
Dr. Andrea Parker is the former chief scientific officer at Peter Munk Cardiac Center, University Health Network. Parker is a clinical epidemiologist with more than 30 years’ experience in clinical trials design, management, and execution in industry and academic settings.
John A. Geddes – Vice-president, Business Development
John Geddes has over 25 years of experience in the healthcare industry, comprising roles within pharmaceutical, biotechnology, clinical diagnostics, and life science research technology companies. Geddes has an MBA degree and is the former corporate senior director of business development at Luminex Corporation, a DiaSorin Company.
Anne Tomalin – Director of Regulatory and Quality
Anne Tomalin is the founder of CanReg and TPIreg, regulatory firms previously sold to Optum Insight and Innomar Strategies, respectively. Tomalin is an expert in regulatory affairs in Canada, the United States, and Europe.
Blagoya Ristevski – Director of Chemical Engineering and Manufacturing
Blagoja Ristevski graduated with a BSc in chemical engineering and inorganic chemistry from the University of Ss ‘Cyril and Methodius’, Skopje, Macedonia, and pursued postgraduate research on natural biopolymers as drug carriers at King’s College London, UK. For 20 years, he was involved in the research and discovery of active drug molecules, drug delivery technologies, and manufacturing methodologies for finished drug products at several biopharmaceutical companies.
Board of Directors
Guillermo Torre-Amione – Chairman
Guillermo Torre is the president of TecSalud academic medical center and school of the Instituto Tecnológico y de Estudios Superiores de Monterrey (ITESM), Mexico. He is the former director of Cardiac Transplantation at the Houston Methodist DeBakey Heart & Vascular Center.
Jennifer M. Chao – Director
Jennifer M. Chao has over 25 years of experience in the biotech and life sciences industries focused primarily on finance and corporate strategy. Chao is managing partner of CoreStrategies Management, a company she founded in 2008 to provide transformational corporate and financial strategies to biotech/life science companies for maximizing core valuation.
Peter Pekos – Director
President and CEO at Dalton Pharma, Peter Pekos has broad experience in research, development, and commercialization of pharmaceuticals, products, and services.
Colin Stott – Director
Colin Stott has over 30 years of experience in pre-clinical and clinical development, with specific expertise in the development of cannabinoid-based medicines. Stott is the chief operating officer of Alterola Biotech Inc. and the former scientific affairs director, international, and research and development operations director for GW Pharmaceuticals, a world leader in the development of cannabinoid therapeutics.
Teri Loxam – Director
Teri Loxam has over 25 years of experience in the pharmaceutical, life sciences and TMT industries with diverse roles spanning strategy, investor relations, finance and communications.. Loxam will be the chief financial officer of Compass Pathways plc (Nasdaq: CMPS), a biotechnology company dedicated to accelerating patient access to evidence-based innovation in mental health.
Michael Willner – Director
Michael Willner has practiced as an attorney and a certified public accountant. He graduated from Emory University Law School as a member of the Emory Law Review. Subsequently, he practiced real estate and corporate law with New York City-based Milbank, Tweed, Hadley & McCloy, one of the nation’s most prominent international law firms. Before his legal career, Willner was employed by the former Arthur Andersen & Company, a national accounting firm, where he practiced in the tax department.
Scientific Advisory Board
Dr. Paul Ridker
Dr. Paul Ridker is director of the Center for Cardiovascular Disease Prevention, a translational research unit at Brigham and Women’s Hospital in Boston (BWH). A cardiovascular medicine specialist, he is also the Eugene Braunwald Professor of Medicine at Harvard School of Medicine (HSM). Ridker received his medical degree from HSM and then completed an internal medicine residency and a cardiology fellowship at BWH. He is board certified in internal medicine. Ridker’s clinical interests include coronary artery disease and the underlying causes and prevention of atherosclerotic disease. He is the author of over 900 peer-reviewed publications and reviews, 64 book chapters, and six textbooks related to cardiovascular medicine.
Dr. Bruce McManus
Dr. Bruce McManus is a professor emeritus of the Department of Pathology and Laboratory Medicine at the University of British Columbia. He has served as CEO of the Center of Excellence for Prevention of Organ Failure (PROOF Center), director of the UBC Center for Heart and Lung Innovation, and scientific director of the Institute of Circulatory and Respiratory Health, CIHR. McManus received BA and MD degrees from the University of Saskatchewan, an MSc from Pennsylvania State University, and a PhD from the University of Toledo. McManus pursued post-doctoral fellowships at the University of California, Santa Barbara in environmental physiology and at the National Heart, Lung, and Blood Institute in Bethesda. McManus served as MD in cardiovascular and pulmonary pathology, and completed residency training at the Peter Bent Brigham Hospital, Harvard University, in Internal Medicine and Pathology.
Dr. Joseph Hill
Dr. Joseph Hill is a professor of internal medicine and molecular biology, chief of cardiology at UT Southwestern Medical Center, in Dallas, and is the director of the Harry S. Moss Heart Center. Hill holds both the James T. Willerson, MD, distinguished chair in cardiovascular diseases, and the Frank M. Ryburn Jr. Chair in Heart Research. He graduated from Duke University with an MD and a PhD in 1987. Hill’s PhD dissertation research was in the field of cardiac ion channel biophysics. He then worked for five years as a postdoctoral fellow at the Institut Pasteur in Paris, studying central and peripheral nicotinic receptors. He next completed an internal medicine internship and residency, as well as a clinical cardiology fellowship, at the Brigham and Women’s Hospital, Harvard Medical School.
Credit: Source link